Recognition of Knee Injury
There are several types of knee injuries that may occur and are common due to running. Read the information below to try and decide what type of knee injury the runner in our case may have.
Objectives:
Upon completion of this section of the module the learner will:
1. State what types of knee injuries may occur with running with 80% accuracy.
2. Differentiate between the types of knee injuries that may occur with running with 80% accuracy.
3. State what signs and symptoms are characteristic of each type of injury with 80% accuracy.
|
Patellofemoral Pain Syndrome (Runner's Knee)
The Patella, or kneecap, is a bone located in the center of the front part of the knee. It acts as a leverage point for the muscles on the top of the thigh, the quadriceps (McGee, 2009). Normally, the patella tracks both inferiorly and superiorly and medially and laterally in the trochlear groove and intracondylar notch, which is formed by the medial and lateral condyles of the femur (inside and outside of the leg bone--see Figure 1) (McGee, 2009). Alterations of this tracking may be caused by muscle imbalances around the knee such as a tight tensor fasciae latae (a muscle that attaches on the outside of the leg that brings the leg out to the side, straightens the knee or flexes the knee depending on hip position), a weak vastus medialis muscle (one of the quadriceps muscles), an overly strong vastus lateralis muscle (one of the quadriceps muscles), or a tight rectus femoris (McGee, 2009). As these muscles act on the joint and pull the patella laterally, abnormal forces are created in the articulation. As these forces act, pain develops (McGee, 2009). Additional causes of this type of syndrome may be due to over pronation of the foot, abnormalities in the joint or other bony structures, or overuse. Overuse develops due to increased forces around the knee joint, and is most commonly due to chronic overloading (running too much) (McGee, 2009). Common signs and symptoms of this type of injury are "pain that is diffuse and arises from the anterior aspect of the knee" (McGee, 2009, p.616). Pain is often produced by activity and increased by squatting, inclined walking, prolonged sitting, and ascending and descending stairs. A person may also report pain along the middle and outer parts of the kneecap, pain behind the knee cap, or a snapping or popping sound with bending of the knee. Onset of this pain is often slow and insidious, however, overuse may decrease the time to onset of symptoms. (McGee, 2009, p. 617). |
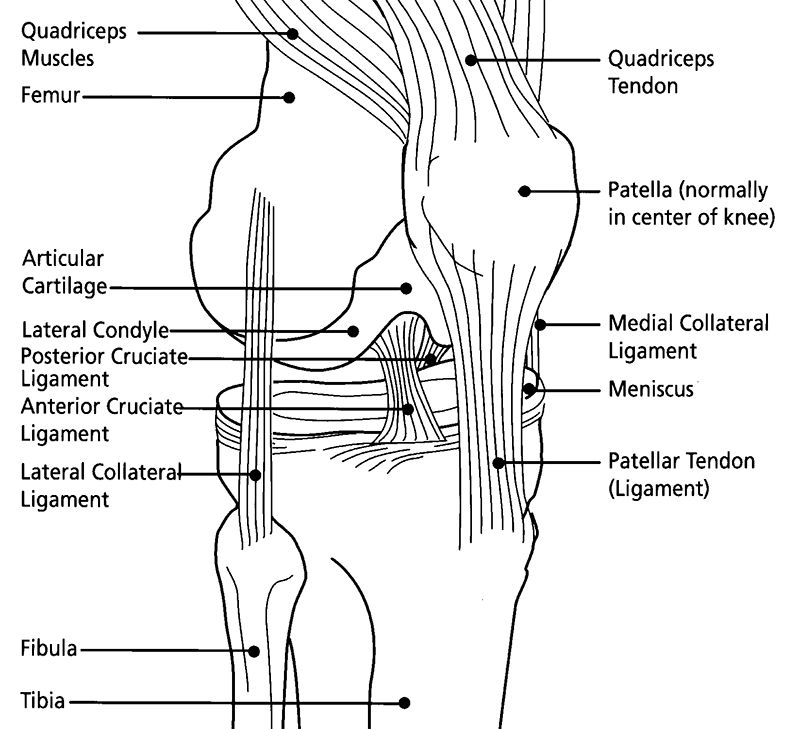
Figure 1, Public Domain, via Wikimedia Commons
|
Meniscal InjuryThe menisci are two cartilaginous (made of cartilage) structures that attach to the tibia (the lower leg bone). There are two, a medial meniscus and a lateral meniscus. The medial meniscus is C-shaped, whereas the lateral meniscus is semicircular. These structures help with distributing weight across the tibia, decreasing joint stress, provide shock absorption and passive joint stability, and limit motion within the knee (McGee, 2009).
Persons with history of meniscus tears usually have a mechanism of injury or history of injury caused with weight bearing, twisting of the knee, or bending the knee to end range of motion (McGee, 2009). Meniscal injury may also occur as a result of degeneration in individuals over the age of 40 (McGee, 2009). Types of injury to the meniscus are pictured to the right from b-e. Both types of meniscal injury present with joint line tenderness (pain where the knee bends), minimal to moderate swelling, pain with bending of the knee, and decreased ability to straighten the knee (McGee, 2009). Lateral Meniscus Lateral meniscus tears present with pain on the outside of the knee where the joint bends (at the joint line). Medial Meniscus Medial meniscus tears present with pain on the inside of the knee where the joint bends (at the joint line). |

By Stündle (Own work) [CC0], via Wikimedia Commons
|
Stress FracturesA stress fracture is caused due to the "inability of the bone to withstand repetitive bouts of mechanical loading" (McGee, 2009, p. 685), meaning that the bone is unable to tolerate the repetitive stresses placed on it. Individuals who run, jog, or sprint seem to have more risk of stress fractures.
Stress fractures occur due to overuse or overtraining. Another cause can be a rapid change in training type or a dramatic increase in the number of training sessions, however, this varies from person to person (McGee, 2009). In addition, road running or worn out shoes or shoe inserts have been shown contribute to stress fractures. Other causes of these injuries could be due to poor bone density, weakened muscles, restriction in joint range of motion, previous low levels of fitness, female gender, and poor nutrition (McGee, 2009). The most common sites of stress fractures are the tibia, metatarsals, and fibula (McGee, 2009, p. 687). Stress fractures will present with a gradual onset of pain with activity that occurs at a specific point in exercise. The pain will progress over time or become more severe as the fracture becomes worse. When touched, or palpated, the bone will be locally tender. In addition, localized swelling, warmth, or redness may be present (McGee, 2009). A stress fracture will be confirmed by imaging. |
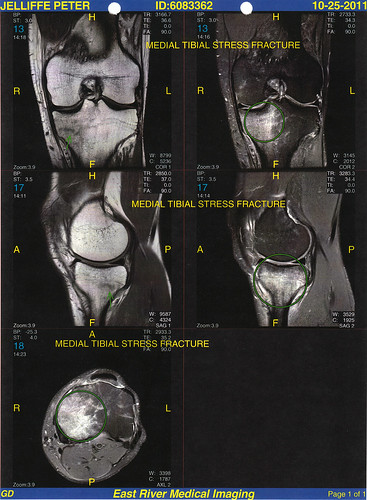
Medial Tibial Stress Fracture from: PetroleumJelliffe on Flickr
|
Muscle or Soft Tissue InjurySprain
Sprains of the collateral ligaments are most likely due to a quick change in direction from side to side while running (Greishamer and Kelly, 2007). Medial Collateral Ligament The medial collateral ligament of the knee is located on the inside of the knee and connects the femur to the tibia (Figure 1)(Brunnstrom, 1999). This type of injury is usually due to having a valgus (knee being pushed in while foot goes out) force exerted to a weight bearing knee (McGee, 2009). Individuals with this type of injury often report being hit on the lateral (outside) side of the knee while the foot is planted. A pop may be heard, however, most often, a tearing sensation will be felt on the middle (medial) side of the knee (McGee, 2009). Swelling occurs quickly with this injury, and individuals walk with a limp and with the knee bent (McGee, 2009). Lateral Collateral Ligament The lateral collateral ligament of the knee is located on the outside of the knee and connects the femur to the fibula (Figure 1) (Brunnstrom, 1999). This type of injury is due to impact, does not usually result in swelling, and is associated with pain on the lateral side of the knee. A pop is usually heard with disruption of the ligament (McGee, 2009). This type of injury is uncommon, and usually does not occur with running. Strain Muscle strains generally occur due to overuse or due to an overly forceful contraction. These are most common in runners who perform ballistic movements such as sprinting. Another cause of strains can be muscle shortening or imbalance as a result of tight musculature (McGee, 2009). Hamstring The hamstring muscles bend the knee and extend the hip. A strain of the hamstring muscles (semimembranosis, semitendinosis, and biceps femoris) presents with pain with extension of the leg or flexion of the knee. These are caused by overuse or poor eccentric (the muscle has to control lengthening) control during sprinting (McGee, 2009). Another cause of strains can be imbalance as a result of tight musculature around the hip joint (McGee, 2009). Hip Flexor The hip flexor muscles (iliopsoas and rectus femoris) bend the hip forward or bring the leg up. The rectus femoris also helps to straighten the knee. A strain of the hip flexor muscles can occur in the anterior thigh or hip usually due to quick movements such as sprinting. Signs of this injury include pain in the front of the leg with active motion of the hip forward or upward (Heck, 2013). Iliotibial Band Syndrome Iliotibial band syndrome is caused by a tight iliotibial band (iliotibial tract as noted in diagram to the right) rubbing against the lateral femoral condyle at the knee. It is common in runners due to the use of this muscle to stabilize the hip while the runner is on one leg during the running cycle. Pain from this type of injury is localized to the lateral (outside) portion of the knee above the joint (lateral epicondyle of the femur) (McGee, 2009, p. 618). A person with this type of injury will often report a snapping sound or feeling of snapping over the outside of the knee joint when the knee is slightly bent. |
Click to set custom HTML

By Kari Stammen (Sent to me personally) [Public domain], via Wikimedia Commons

By Beth O'Hara via wikimedia commons through CC-BY-SA-3.0-migrated license
|
Self Check Quiz
|
References
Content written by Nancy Smith, PT, DPT, GCS; images courtesy of wikimedia commons.
1. Brunnström, S. (1996). Brunnstrom's Clinical Kinesiology revised by Smith K, Weiss E, and Lehmkuhl D. Philadelphia, PA: Davis.
2. Greisamer, RP and Kelly FB (2007, August). Knee and lower leg. http://orthoinfo.aaos.org/menus/leg.cfm. Retrieved April 1, 2013 from http://orthoinfo.aaos.org/menus/leg.cfm.
3. Heck, Jon. Hip flexor strain. http://www.stockton.edu/ospreys/HipFlexorStrain.htm. Retrieved April 1, 2013 from http://www.stockton.edu/ospreys/HipFlexorStrain.htm.
4. Magee, D. J., Zachazewski, J. E., & Quillen, W. S. (2008). Pathology and intervention in musculoskeletal rehabilitation. Saunders.
5. Salter, R. B. (1999). Textbook of disorders and injuries of the musculoskeletal system: an introduction to orthopaedics, fractures and joint injuries, rheumatology, metabolic bone disease, and rehabilitation. Williams & Wilkins.
1. Brunnström, S. (1996). Brunnstrom's Clinical Kinesiology revised by Smith K, Weiss E, and Lehmkuhl D. Philadelphia, PA: Davis.
2. Greisamer, RP and Kelly FB (2007, August). Knee and lower leg. http://orthoinfo.aaos.org/menus/leg.cfm. Retrieved April 1, 2013 from http://orthoinfo.aaos.org/menus/leg.cfm.
3. Heck, Jon. Hip flexor strain. http://www.stockton.edu/ospreys/HipFlexorStrain.htm. Retrieved April 1, 2013 from http://www.stockton.edu/ospreys/HipFlexorStrain.htm.
4. Magee, D. J., Zachazewski, J. E., & Quillen, W. S. (2008). Pathology and intervention in musculoskeletal rehabilitation. Saunders.
5. Salter, R. B. (1999). Textbook of disorders and injuries of the musculoskeletal system: an introduction to orthopaedics, fractures and joint injuries, rheumatology, metabolic bone disease, and rehabilitation. Williams & Wilkins.